Asthma is a common disease and presents to acute healthcare services extremely frequently.
The majority of presentations are mild exacerbations of a known diagnosis and are relatively simple to assess and treat, many being completely appropriate for out patient treatment. On the other hand around 200 deaths per year are attributable in the UK to asthma, and therefore in the relatively young group of patients there is a real potential for critical illness with catastrophic consequence if not treated effectively. The majority of these deaths occur prior to the patient making it to hospital making the prehospital phase extremely important and hugely stressful in these cases.
It is also worth noting that of the deaths reported that many were associated with inadequate inhaled corticosteroids or steroid tablets and inadequate follow up, meaning that our encounter with these patients at all stages of their care even if not that severe at the point of assessment is a key opportunity to discuss and educate about treatment plans and reasons to return.
In Part 1 of the podcast we’ll run through
- Pathophysiology
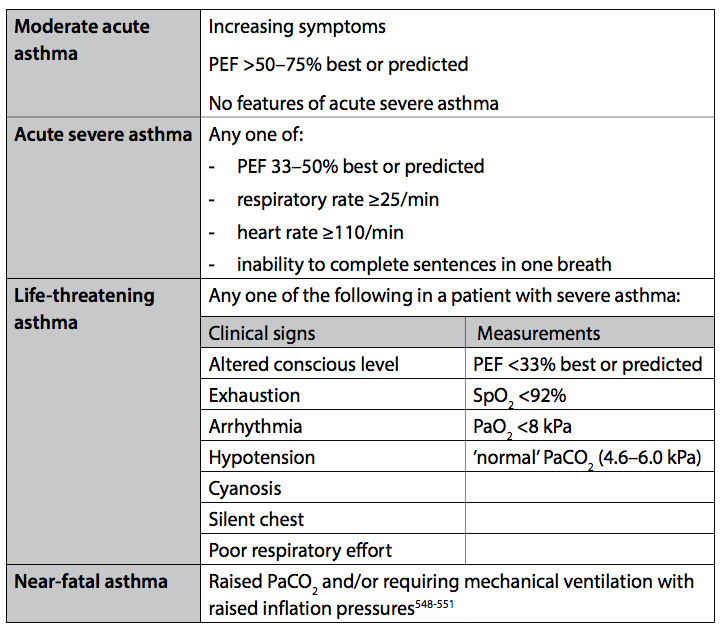
- How patients present
- Guidelines
-
- Salbutamol
- Ipratropium
- Steroids
- MagnesiumTreatment
-
Part 2 covers
- Ketamine
- Ultrasound in asthma
- NIV in asthma
- Asthma related cardiac arrest
- Imaging
- Management
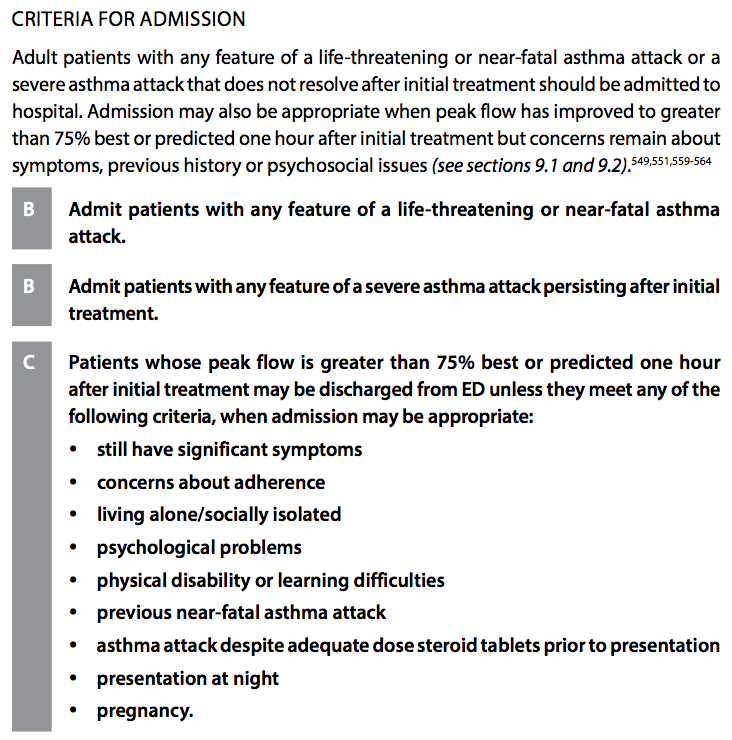
- Discharge
We hope you enjoy it and would love to hear your feedback!
Detection of pneumothoraces in patients with multiple blunt trauma: use and limitations of eFAST. Sauter TC. Emerg Med J. 2017
TheResusRoom; Needle Thoracostomy podcast
TheResusRoom; BTS Asthma Guidelines 2016 podcast
LITFL; Non-invasive ventilation (NIV) and asthma
Intensiveblog; Asthma mechanical Ventilation Pitfalls
Australian Asthma Handbook; Quick Reference Guide
BTS Asthma Severity Criteria
BTS Admission Criteria